Bones are the most important structure in the human frame which allows us to create movement, generate and store calcium, withstand significant force and create growth. Below identifies many different aspects of the bone which would need to be accounted for.
TYPES OF TISSUE IN THE BONE:
CORTICAL:
Cortical bone is seen within the diaphysis of the bone as the middle of the bone is the part which withstands the most pressure and would be most vulnerable to fractures. Cortical bone is sometimes known as 'Dense bone' due to the thickness of its structure. The bone has to renew every 10 years to prevent deterioration. The cortical bone is made up of mostly natural compounds such as calcium and collagen.
CANCELLOUS:
Cancellous bone is the complete opposite in terms of structure compared to cortical bone, it is seen to be a spongy bone, thus that term has become a nickname for the bone. The spongy bone has a similar resemble to a honeycomb structure, this allows nerves and blood vessels to passage through the holes in the structure to give the bone the oxygen and nutrients it needs to keep its strength.
ASPECTS OF THE BONE:
EPIPHYSIS:
Seen at the ends of the bone, there are two epiphysis situated on the bone, these are known as the proximal and distal epiphysis. The epiphysis is where cancellous bone would most frequently be found. The epiphysis is made up of the epiphysis plate and line, both of which help promote ossification. The epiphyeal plate is made up of hyaline cartilage and is the part of the bone which grows during childhood, the epiphyeal line shows the 'leftovers' of the epiphyeal plate in adulthood.
DIAPHYSIS:
The diaphysis is situated in the shaft of the bone and contains cortical bone, the most important job this bone is used for is to store yellow bone marrow which in adults stores fat, this can help promote red blood cell production.
TYPES OF BONE:
Long bone: Long bones are the most common types of bone in the body, the length of the bone is significantly bigger than the width of it, thus the name 'long bone'. These bones can be found in fingers and toes (metacarpals/tarsals), radius, ulna, femur, humerus.
Short bone: Short bones consist of a body which is larger in width compared to its length, they promote support and structure of the wrists and the ankles for example, the most common types of short bones would be the carpal and tarsals in the wrists and ankles.
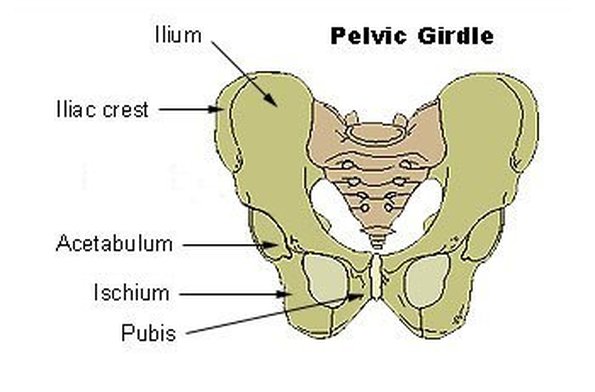
Flat bone: Flat bones are most obviously flat, they're used for protection of vital organs as they're usually rather large and consist of a thick layer of cortical bone. Examples of the flat bone are the scapula, the skull and the hip (illium)
Sesamoid bone: The sesamoid bone is found imbedded between two tendons, these are present most often next to joints as it serves as protection for the tendon which could come into contact with the moving joint. An example is the patella (knee bone)
Irregular bone:The answer is in the title, irregular bones are bones which don't fall into any other category because it's of an irregular shape. Examples include the Sacrum (end of spinal column), Vertabrae found in the spinal column and the mandible (lower jaw)
BONE STRUCTURE #2
Periosteum: It is a double layer membrane which makes up the outer sheet of the bone tissue, it is significant as it is supplied with blood vessels, nerves and lympatic vessels.
Endosteum: This is the inner layer of the bone surface, this is where osteocytes are present meaning that this is where osteoblasts and osteoclasts work in order to maintain appropriate levels of collagen and calcium levels.
BONE CELLS
Both osteoblast and clasts are used prodominantly for ossification (bone remodeling) and can be found in the endosteum (cortical bone).
Osteoclasts: The first stage of bone remodelling occurs when osteoclasts begin to remove and reabsorb bone tissue found in the endosteum, this tissue would have been deprived of collagen meaning it would need to be removed in order for new collagen to be injected into the tissue.
Osteoblasts: The second stage is when the osteblasts move into lay down new bone tissue full of collagen, the new bone tissue would be layed upon the osteocytes which had previously been stripped by the osteoclasts.
INJURY CONCERNS OF THE BONE
Avulsion fractures: Avulsion fractures are commonly caused by stress placed upon a certain bone, this means that the bone remodeling cannot cope with the ongoing demands of the bone wanting to become stronger.
Spondylolysis: This is most often seen in the vertabrae and it's the degeneative osteoartheritis of the spinal vertebrae coming together. It is sometimes referred to as the 'spotty dog' due to its resemblance of a dogs collar.
Osgood Schlatters Disease: A problem which occurs in the knee, it is the pain and swelling of the ligament due to the inaccurate growth of the eiphyseal plate.
Severs disease: A fracture which occurs in the heel bone, it is most commonly seen in children. It is the inflammation and fracture of the calcaneus which is caused by the achillis tendon pulling too hard on the attachment which is situated on the calcaneus.
Salter Harris fracture: This results in a fracture taking place in the epiphyseal plate which will cause deformation of the plate and also causes the the plate to close off preventing any further growth in the epiphysis.